|
|||||
|
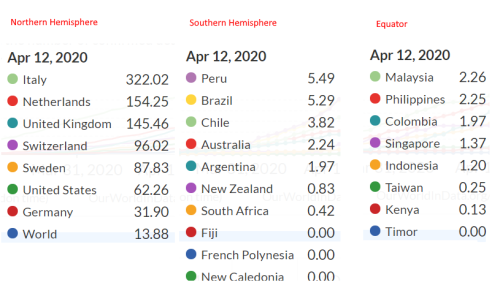
Dear , With Easter out of the way I wanted to put some perspective on the COVID-19 situation and how the Australian government is handling it, but first an up-date on our court action against the Electoral Commission. AIP v ECQ I understand that the Electoral Commissioner is likely to seek costs. While this is not unexpected, and he may have a legal right, I don't think he has an ethical right. The commissioner was giving bad advice to donors and organisations and denying them their democratic right of participation. He was right to say they couldn't donate for electoral expenditure, but wrong to say they couldn't donate to organisations that incur electoral expenditure. In running this case we've done other organisations like ours a favour, and we've also done the commission a favour. I'll keep you informed. COVID-19 We appear to have 7 Australian governments that are paralysed, unable to decide whether they are really "flattening the curve", which means spreading the same number of infections out over a longer period of time, or "obliterating the curve", meaning eliminating the virus altogether. While they are still talking about "flattening the curve" they appear to want to have eliminated new infections before they start relaxing restrictions, and that's a confusing message, and a recipe for long term disaster because it envisages a series of lockdowns. Proper flattening of the curve meant only one real lockdown. Primacy of the disease over everything elseThe first thing I want to comment on is the primacy that we are giving this disease and what appears to be a radical reshaping of our tolerance of risk. We live and work with diseases that kill some of us, and that we infect each other with, all the time. Generally we don't shut the economy down because of a flu epidemic, although we did a hundred years ago with Spanish Flu, but that is a very rare event. This pandemic is not the Black Death, which killed somewhere around half of Europe, and probably not even the Spanish Flu, which killed perhaps 1% of the world's population. The first reports I saw suggested a mortality rate as high as 20% and a rate of transmission as high as 5. That warranted strong interventions. Flattening the curve was a real imperative, but once we got the logistics sorted to enable the overload of cases to be hospitalised, the only viable plan seemed to be to go back to work and take our chances with the disease, as we always have. But that's not what we are doing. How good is Australia's performance?We appear to have one of the best performances in the world when you look at fatalities. The table below measures the fatalities per million. It gives you some comparisons, but it also should raise some significant questions, like why the death rate is so low in the southern hemisphere.
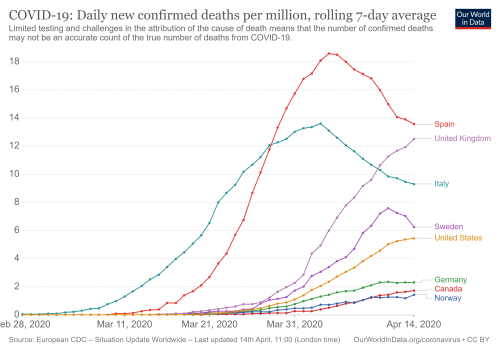
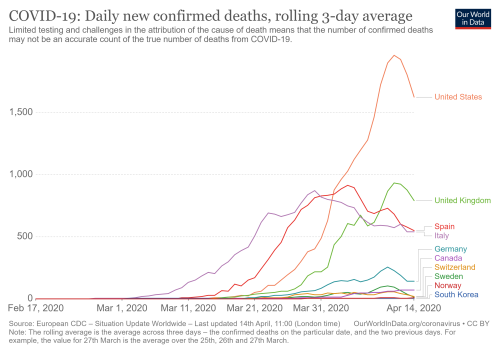
It might be that infections arrived here later, and we learned from others and took better precautions. Maybe, but surely not all those countries in the right hand two columns could be that superior to their northern cousins. Or it might be that it is not our flu season yet, and it is Europe's, or that the virus does not like higher temperatures. Another thing you can see from this is that Sweden, which has kept open through all of this, is not doing too badly, for a northern hemisphere country. It certainly doesn't have a death rate that deserves the derision it has been receiving. How dangerous is COVID-19?If you get it into your lungs, and it triggers an auto-immune reaction, it is very serious, causing pneumonia. Otherwise it appears to be not so serious, and many people get such a mild dose they don't realise they've had it. The flu also causes pneumonia, but has a reproductive rate (the number of person one person will infect) between 0.9 and 2.1 and fatality rate of about 0.1%. COVID-19 has a reproductive rate of somewhere between 1.4 and 5.7 and a fatality rate that the Queensland government puts at 1%, but WHO puts at 3.5%. You might have noticed that the figures for the flu come with a smaller spread than COVID-19. That's because we still really don't know enough about this disease to be very accurate. So it is no wonder that the various models come to different answers, and in most cases seem to have over-estimated the severity of the outbreak by orders of magnitude. As the latest from Professor John Ioannidis suggests, fatality rates may be nowhere near as high as suggested because the disease is probably more prevalent in the community than we realise. While over-flowing ICU rooms suggest the disease is rampant, with such a high potential reproductive rate, you would expect the disease to peak very quickly and then die just as quickly because it would exhaust the pool of potential victims earlier. While flu cases are more likely to be spread over a long period, you'll see more COVID-19 cases earlier, which could mean fewer later, and a similar rate over the course of a year. But the only way we can get a handle on this is by testing representative samples of communities so we pick up people who are asymptomatic, as well as those who have recovered. With some exceptions that testing is not happening. But if warmer weather suppresses the virus, then you might see fewer ealier on, and then a surge once you get into colder weather in winter. Perhaps the effects of the disease are also milder in warmer weather. In which case Australia's figures may be nothing to boast about and merely the prelude to the storm. In which case we could have allowed it to spread before the flu season using the climate as a natural moderator on its initial severity.. Are enough people getting sick?This is the core of my concern, and I understand is challenging for those who have characteristics that make them more likely to catch the disease, but needs to be talked about nevertheless. When you look at the statistics for Sweden, which has been criticised for not locking-down, its figures are now dramatically improving. The first chart below shows a rolling 7 day count of deaths per million, while the second shows a rolling 3 day count of deaths. While things were pretty dire in Italy and Spain their numbers are coming down, and they should be able to go back to normal, more or less COVID-free, in a fairly short time. The same applies to Sweden. Unless Australia loosens up its restrictions, it won't apply to us.
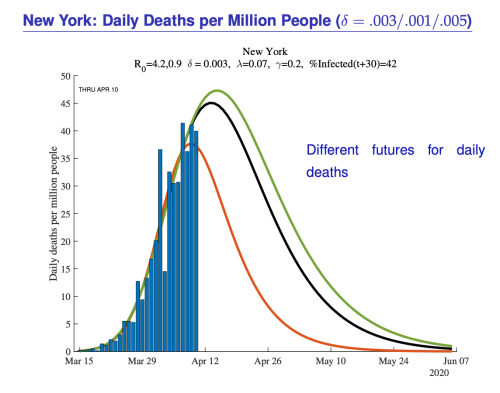
Some of those curves look pretty similar to the ones being predicted for New York by Jesús Fernández-Villaverde and Chad Jones, which I sourced from The Grumpy Economist.
The death rate might look high, but what needs to be taken into account is what happens over a longer period, say a year. It is impossible to know, but given the average age of people succumbing at over 80 years of age, there is a good chance that many might not have made it through a twelve month period in any event. How many deaths is too many?The last thought I want to leave you with is the implicit trade-off that we are making when we prioritise something above almost everything else - in this case treatment of people with COVID-19. It means that something else has to be neglected. Even with the low level of infection in Australia there has been a huge diversion of resources towards a potential inundation of COVID cases. If the inundation had arrived, then there would have been a further diversion of resources. As the curves above demonstrate, this would probably have been for an intense two month period. We've traded the two months off against something much longer. In the process we have also shut the economy down, unlike a number of other countries like Sweden, Singapore, Japan and South Korea. Shutting the economy down pushes costs away from those most likely to get COVID, to those less likely, which includes people in the workforce. We tend to think of the death rate from the virus in absolute terms - it has killed x number of people. A more sophisticated way of looking at it, but much harder to accurately gauge, is that it has shortened their lives. When you look at mortality rates through the lens of lifespan, they look entirely different. So if a young person commits suicide because of the depression we are creating to fight COVID, then his length of life foregone could be many multiples of the average victim, who is aged over 80. Added to that are quality of life issues. What if the 80 year old has dementia and is bed-ridden? And then there is the general shortening of life that poverty causes. So a depression will cause younger people to have a shorter life than they otherwise would, in a mirror reflection of the shortening of life of older people. It's not happening at the same time, but it is happening nevertheless. Paul Fritjers has put these issues and more together in a concept called WELLBYS, which he blogs about here. He concludes: So however I look at it, it seems clear that the unemployment and emotional costs of mass social isolation far outweigh the threat of the virus and the immediate lifting of nearly all involuntary isolations is warranted. It is not "safe" to keep the isolations in place. ConclusionWhen we started on this crisis the government should have had more information than the rest of us because they have commonwealth bureaucrats who had presumably done some planning for the eventuality of a pandemic. We were in a fog of war, and they struck out with what seemed a clear strategy - seal off the country and control the rate of infection so that the infrastructure could deal with it, while a significant proportion of us caught the disease. Here we are a little way in, and it is clear that they've changed their strategy. They either think they can eliminate the virus without most of us catching it first, or they don't think we are prepared to accept the fatality rates that would go with the first strategy. Whatever way it is, there is a clear failure to discuss how this pandemic is to end in Australia, and what costs we should be prepared to bear. All that is happening is that each state is getting more and more hairy-chested about imposing stricter and stricter limitations on personal limits, and in some cases confiscating private property rights, and the public's focus is just on the daily infection figures, as the progress of the disease is being called by journalists like a slow-moving Melbourne Cup. That is not good enough. No one anywhere, government or opposition, state and federal, or health bureaucrats, is showing any sort of leadership. This is a crisis where muddling through is the only policy response, and the fatalities will be counted long after the virus has disappeared. Regards, |
||
|
|||||